
X-rays and Hair Removal
Within a year of Wilhelm Roentgen’s 1895 discovery of a new form of radiation, that he called X-rays, the medical profession was using them for therapeutic as well as diagnostic purposes. Their first reported use in dermatology occurred in 1896 when Leopold Freund – the Viennese founder of radiotherapy – deployed them to treat a large hairy growth covering the entire back of a patient. After twelve days of treatments, during which the patient was exposed to 20 hours of X-rays, the hair on the growth began to fall out. The report on the case in 1901 began a long medical interest in using X-rays to treat hypertrichosis and other forms of excess hair.
Hypertrichosis, hirsutism & superfluous hair
Hypertrichosis – abnormal or excessive hair growth – is a medical condition with a number of causes, including genetics, abnormal skin growths and skin trauma. A second medical condition that can produce excessive hair in women and children, referred to as hirsutism, is the result of abnormally high levels of androgen hormones.
Some women who did not suffer from either of these conditions also sought medical treatment for what is known as superfluous hair, typified by the darker hairs on the upper lips of women of Middle Eastern or Mediterranean origins and when these women emigrated to places such as America or Australia they often sought treatment to remove it.
Electrolysis
There are numerous methods for temporarily getting rid of excess hair but before X-rays the only recognized procedure for permanently removing hair was electrolysis. First used in 1875 to remove problem eyelashes it had become widely accepted by the medical practice as the safest and surest treatment by the 1890s. Unfortunately, it was slow, painful and expensive, making it less than suitable for treating large areas of the body.
See also: Electrolysis
X-rays
The medical profession enthusiastically adopted X-rays to treat a large array of skin complaints including acne, eczema and lupus vulgaris even though the rays were shown to be capable of causing skin burns, dermatitis and cancerous growths (Wolbach, 1909). Although some condemned the treatments, many practitioners of the time thought that these and other problems were the result of bad practices that had occurred when X-rays were new and poorly understood. They believed that the use of screens, shorter exposure times and generally improved techniques would reduce the risk of the more serious consequences and noted that cases in which patients were harmed were decreasing rapidly. Unfortunately, the medium-term and long-term effects of X-rays would not become generally apparent until the 1920s.
X-rays were also used by the medical profession to remove hair. For example, children suffering from ringworm or other forms of fungal infections were often subjected to X-rays to remove infected hair as part of the treatment for the condition. Doctors at the time thought that removing the hair withX-rays were preferable to other, more painful epilation techniques such as forceps or hot wax.
See also: Epilation Wax
X-rays were also used medically to induce permanent hair loss in patients suffering from hypertrichosis. When used in temporary hair removal – such as in patients with ringworm – the immediate (acute) consequences of X-rays could be partially controlled. However, if X-rays were used to produced permanent hair loss this required higher doses of the ray resulting in changes in skin pigmentation as well as thickening, redness, telangiectasia and dermatitis.
In ordinary cases of hypertrichosis we regard electrolysis as the safest and surest method, but in some severe cases which cannot be treated in this way X-rays hold out the only hope of amelioration. Patients must be warned not only of the possibility of dermatitis, but also of the late appearance of pigmentation, atrophy, and telangiectasis. On account of these sequelae, results which appear highly successful at first may eventually prove to be anything but satisfactory. Most observers agree that the removal of downy hair is difficult, and, on the other hand, cases may occur in which strong, coarse hairs cannot be removed—without giving a larger dose than the skin of the face which is more sensitive than that of the scalp—is able to bear without dermatitis. The majority of reported cases have been treated with small repeated doses, smaller doses being required after epilation has occurred to prevent recurrence. Some authors prefer to give a full dose of 3 or 4 H., varied according to the sensitiveness of the skin short exposures of five to ten minutes being given subsequently about every two months to prevent re-growth.
(Morris & Dore, 1907, pp. 225-226)
It is a testament to the desire of clients to lose their excess hair that many would accept these harmful side effects.
In one case, a male, a music teacher, was desirous of having all of the hairs removed from the forearms and the backs of his hands during the summer vacation. This patient was made aware of the dangers connected with such heroic treatment. The right forearm and back of the hand was a complete success. All of the hairs fell out after the fourth exposure, the erythema was marked, but at no time required any particular attention. The left forearm having received as nearly as possible the same amount of raying, showed a decided erythema, which in some places destroyed the superficial skin and upon healing showed that typical scar which is the result of a Roentgen ray dermatitis. While this patient declared himself as perfectly satisfied, such a condition is not desirable upon the face.
(Geysee, 1915, p. 521)
Given the problems with X-ray burns and other dangers any development which was likely to reduce risk was warmly received.
Albert Geyser
In 1908, Albert Geyser demonstrated his new Cornell X-ray tube at a meeting of the New York Physical Therapy Society. Named after the Cornell University Medical College, where he was based, Geyser claimed that the Cornell tube eliminated many of the dangers associated with the use of X-rays, including X-ray burns.
The Cornell tube is made of heavy lead glass so that no rays are emitted, except through a flint glass window, which corresponds in size to the lesion to be treated. The connecting wires are encased in glass insulators to prevent sparking on any part of the patient while under treatment. The flint glass window is situated at the end of a projector, and must be in direct contact with the lesion, thus furnishing a ground and doing away with the air space which would otherwise be the dielectric between the tube and the patient.
When the tube is brought into direct contact with the patient only the ionizing effect of the X-ray is exerted on the tissue, and this effect is all that is needed to furnish the most brilliant therapeutic results.(New York Times, April 12, 1908)
Although it might have reduced the possibility of inducing burns, and despite the title the New York Times gave its story on the invention, ‘New Tube Robs X-Ray of Danger’, as we now know, the instrument was anything but safe; however, that is to judge it in hindsight. Geyser himself was well aware of the hazards of X-rays – the fingers of his left hand were so badly disfigured by exposure during his experiments that he had been urged to have them amputated – so would not have taken its dangers lightly.
Geyser used his device to treat a range of skin conditions including lupus vulgaris, rodent ulcers and eczema but it was excess hair that became the centre of his attention. Although he was initially critical of using X-rays for removing hair, his opinion on the subject appears to have changed by the end of the First World War. At a meeting recorded in the 1918 Journal of Cutaneous Diseases, when he was asked about his change of heart his reply was recorded as follows:
It did not make any particular difference because he said a certain thing was dangerous, everything was dangerous. Every drug may be dangerous, but the oftener and longer one used it, the greater the experience and results. There was every reason for changing an opinion, and he had shown case after case at this Society and every one of them showed good results.
(Geyser, 1918)
Both Albert Geyser and his son Frank Roebling Geyser – a practising medical physician – conducted numerous X-ray treatments to remove excess hair using the Cornell tube. Presumably, through a combination of trial and error, they developed a standardised treatment regime that they thought would allow them to remove hair without causing dermatitis or other permanent skin reactions. Like other practitioners of the time, Geyser thought current methods of measuring dosage were problematic because they did not take into account the idiosyncrasies of the patients, and that the secret to achieving a good result lay in observing the reaction of the skin of the patient.
Dr. Geyser said the whole secret lay in screening the dose—simply screening sufficiently with aluminum, giving the patient two or three treatments with 2 or 3 milliamperes of current, and if one saw a reaction that came too soon, or no reaction at all, one would not expect to use 5 milliamperes. Only when one could see absolutely no reaction, that was the dose; and if the case were screened more than that, there would be no result, and if less, a dermatitis.
(Geyser, 1918)
It seems clear that Geyser thought that X-rays could be used to produce permanent hair loss with minimal damage to the skin of the client, so long as procedures and machines were standardised and operators periodically checked the skin of their clients to ensure that individual differences did not result an adverse outcome.
At some stage Geyer decided to commercialise what had been learned. In 1920, a business advertised in Philadelphia that it was using the Roebling Geyser Method and this may have been an early licensing attempt on his part. Things got more serious in 1924 when Frank Geyser submitted patent applications for the Cornell tube, first in the United States and then later in Great Britain, France and Germany. These patents would underpin the formation of a commercial enterprise – the Tricho Sales Corporation.
Tricho Sales Corporation
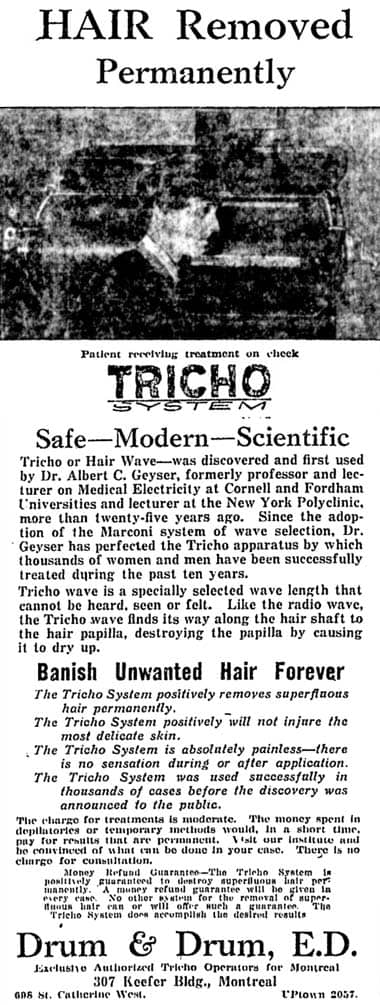
Established in 1924 by a group of investors with Albert Geyser as its Medical Director, the new company was to produce and lease X-ray machines that used the Cornell tube, and to train operators to use them. Operators of the leased machines did not need to be medically qualified and were put through a short course that presumably gave them the basics of how to operate the machine and the treatment courses they were to offer. Tricho Institutes were set up across the United States and abroad, many of which were in beauty establishments. Advertised as the Tricho System, the treatments were branded as being safe, modern and scientific; no mention was made that they used X-rays.
Tricho or Hair Wave—was discovered and first used by Dr. Albert C. Geyser, formerly professor and lecturer on Medical Electricity at Cornell and Fordham Universities and lecturer at the New York Polytechnic, more then twenty-five years ago. Since the adoption of the Marconi system of wave selection, Dr. Geyser has perfected the Tricho apparatus by which thousands of women and men have been successfully treated during the past ten years.
Tricho wave is a specially selected wave length that cannot be heard, seen or felt. Like the radio wave, the Tricho wave finds its way along the hair shaft to the hair papilla, destroying the papilla by causing it to dry up.(Tricho System advertisement, 1926)
Safety
In hindsight, it seems difficult to believe that the widespread use of these machines was possible. However, many other pieces of medical equipment had made the move from medical to lay usage without major harm, electrolysis machines being a case in point. The X-ray machines were considered simple to operate and did not require a skilled technician. In fact, a good case could be made that it required less skill to remove superfluous hair using X-rays than it did by electrolysis.
Also X-rays, if used correctly, were not generally considered dangerous by the medical profession which employed them to treat a wide variety of skin conditions. So, despite the fact that the Tricho Company took out insurance policies to cover themselves for accidental injury, it is likely that Geyser thought his machines were safe.
In his defence, Geyser’s machines did address the main medical concerns of the day regarding X-rays, most of which were related to clients receiving the right dosage. As well a being made of heavy lead glass, the Cornell tube at the heart of the Tricho machine had a square, not a round, window. This allowed the operator to cover the treatment area in a grid fashion, avoiding overlapping and overdosing any part of the skin; something that was criticised in machines where the beam was circular and overlapping was unavoidable. Surrounding screening kept the treatment area localised to the square window, a filter was used to remove the less penetrating ‘soft’ X-rays, and the machine had an automatic cutoff that prevented the operator accidentally exceeding the recommended treatment time. Variation in the distance between the X-ray source and the client was another cause of dosage error but operators of the Tricho machines were told to ensure that clients put their face up against the glass so that the distance between the tube and the skin was correct and that it was the same for all treatments. All of these features reduced the risk of exceeding the intended dosage. Treatment times were also kept short – less than 5 minutes a sitting – to minimise the risk of getting an X-ray burn.
Initial satisfaction
Most of the tens of thousands of women who undertook a Tricho hair removal course were happy with the procedure, the cost and the outcome, at least in the short term. Compared to electrolysis it was fast, painless and effective. The only comparable treatments were those that used radium, which also proved to be unsafe. Investors in the Tricho System were also pleased, clients were plentiful and with fees starting at hundreds of dollars, the system was very lucrative. The New York clinic boasted that it had treated 20,000 cases of superficial hair permanently without a single failure (Collins, 2007).
Medium and long-term effects
This situation only lasted until the medium-term effects of being treated with large doses of X-rays became apparent and clients began to sue. In 1926, Ida E. Thomas took Frank Geyser to the Supreme Court for the $739 cost of her treatments and for an additional $100,000 in damages. Her treatments in his medical practice from 1920 to 1922 had removed her facial hair but had also resulted in her facial skin thickening and wrinkling. In 1925, she declared, her face became swollen and her skin hard and brittle. Other cases followed.
In 1929, the American Medical Association condemned the Tricho treatment for “precancerous keratoses and other untoward effects”. In spite of the evidence Geyser remained defiant, stating that the production of keratoses was “physically and physiologically impossible with the Tricho System” and the “very fact that these machines are installed in beauty parlors and that the beauty parlor public is a hypercritical public, is prima facie evidence that this system of treatment is eminently satisfactory” (AMA, 1929).
Despite Geyser’s protestations, the prospect of being sued for millions of dollars and, I would imagine, the impossibility of obtaining insurance, meant that the Tricho Sales Corporation collapsed in 1930 and was wound up in 1932. Unfortunately, the practice of using X-rays to remove superficial hair continued.
J. M. Marton
Before the Tricho Corporation was formed, others had been at work. From 1914 at least, Jules (or Julius) Marcell Marton had been advertising in newspapers that he could permanently remove hair by the Marton Method. Although he was not a graduate of any reputable medical school or licensed to practice medicine in the United States he was using X-rays to do so.
I do not know what equipment he was using early on but in the 1930s he was using Coolidge Tubes to generate his X-rays. He avoided using the term X-ray in his advertising and literature referring to them by other names such as Epilex-rays or Rœntgen Rays.
The Coolidge Tube; the use of filters to eliminate undesirable rays; the complete control of the electrical current; the perfection of mechanical timers, have all made the use of this machine another great benefaction to mankind.
(Beauty: Woman’s Most Precious Gift, n.d.)
Like Tricho, Marton was sued but unlike them, he did not go out of business. He continued to operate using the technique that had enabled many patent medicine operators to survive in earlier times – move and change your name. Using business names such as Marton Laboratories, Dermic Laboratories, Dermic Institute and Hair-X Laboratories, Marton and his partners continued to operate through the 1930s in the United States and Canada until the businesses he set up were closed down by the authorities (Cleveland, 1948).
One of Marton’s partners in California appears to have been Dr. Henri Eugene St. Pierre [1891-1974]. He was the director of The Dermic Laboratories with branches in San Francisco and Los Angeles. St. Pierre would later develop the Blend Technique of hair removal in conjunction with Arthur Hinkel [1916-1993].
See also: Thermolysis and the Blend
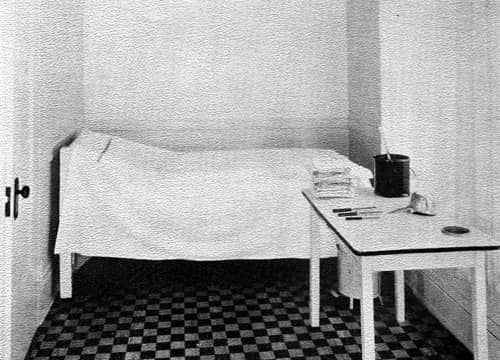
Above: The Dermic Laboratory Epilation Room (San Fransisco) in the 1930s. Clients first had their hair removed using traditional hot wax then the hair follicles were treated with X-rays to prevent regrowth.
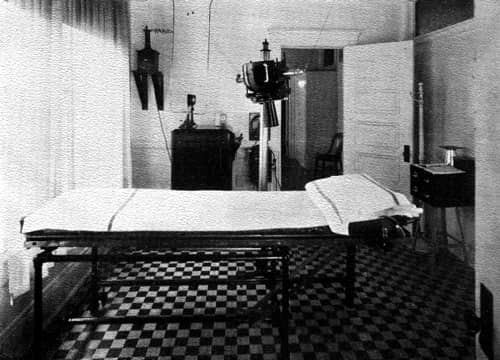
Above: The Dermic Laboratory Rœntgen Ray Room (San Fransisco) in the 1930s. Dermic Laboratories preferred to use the term Rœntgen Ray rather then X-ray. This room appears to have been used to treat body and leg hair.
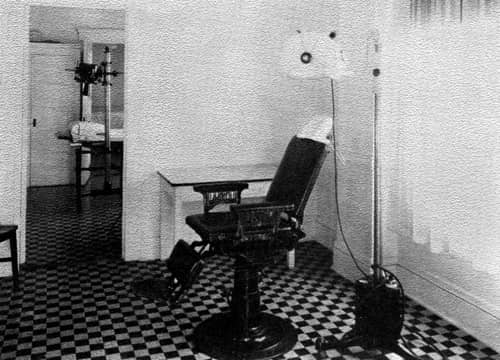
Above: The Dermic Laboratory Rœntgen Room (San Fransisco) in the 1930s. This room was most likely used to treat facial hair.
See also the company brochure: Beauty: Woman’s Most Precious Gift (c.1933)
Consequences
From the 1930s onwards, concerned members of the medical profession tried to put Marton and similar operations out of business. Their objections were mainly due to what could be termed the medium-term effects of X-ray treatments – telangiectasia, skin thickening, scaliness, atrophy, wrinkling, ulcerations and the like – not skin cancer; that would come later. However, they were hampered by the lack of interest of many public health authorities, the secretive nature of the operations, and the lack of ordinances in many jurisdictions that would enable prosecutions to be made. Even if a proprietor was shut down, fines were often small and the machines were not confiscated. This meant they could be moved and/or resold to start up again under a different name and/or location. Devices continued to be on-sold and reused for many years. As the AMA discovered, operators usually had little or no idea about what they were doing and simply followed set procedures. The fact that they were easy to operate was what enabled these machines to be used by non-professionals, with minimal training, in the first place and this now made the job of closing them down more difficult.
Questioned about the machine and her technique, the proprietor had no idea what voltage she was using, said the amperage was “4”, the distance between tube and skin “about 6 or 8 inches”, the time of exposure “about 2 or 3 minutes”, the size of each area treated was “about 4 by 4½ inches”; 10 to 20 treatments at intervals at first of 1 to 10 days and later 2 to 4 weeks constituted a “course”. A filter was used, the thickness and composition of which was unknown.
(Cleveland, 1948)
It is may be true that some operators, particularly in later years, knew they were causing irreparable damage and were just in it for the money, but I think it is more likely that many were ill-informed and thought the treatments were safe.
Cancer
The median interval between X-ray exposure and the diagnosis of skin cancer is 21 years (Martin, Strong & Spiro, 1969) which meant that by the 1940s the long-term effects of using X-rays to treat excess hair and other skin conditions became all too evident, belatedly forcing authorities to act. Unfortunately, closing down all the establishments would take many years as many were run by sole proprietors with clients gained by word of mouth. Articles and reports in newspapers, magazines and books as to the dangerous nature of the treatments helped to cut off business and eventually the last of the machines went out of operation.
Not long ago an unscrupulous person offered a machine guaranteed to remove hair. It was a modification of the X-ray, but as with other frauds, its exact character was secret. The machine could not be purchased; it could be rented only. Physicians, expert in treatment of various diseases by X-ray, report that no X-ray machine can permanently remove hair without at the same time destroying normal surrounding tissue. The very success claimed by quacks practicing hair removal with X-ray proves that the skin has been destroyed, else the hair would grow. … Skin, exposed to X-ray for hair removal, shows signs of destruction sooner or later, by becoming dry, scaly, having enlarged blood vessels, and finally developing a skin cancer. This is not an alarmist statement. It is fact. Many women who submitted to the removal of excess hair by the X-ray method are now being treated by physicians for skin cancer. Many law suits have reached the courts in behalf of women so injured. The court usually awards damages in these cases. Rarely are they collected, for the operator of the machine has either left the jurisdiction of the court or is without funds to satisfy the judgment. He or she does not even own the machine responsible for the damage. The financial loss suffered by the victim is insignificant when compared to the serious damage done to the skin. The skin is far more unsightly than it was with the excess hair.
(Goodman, 1943, pp. 126-127)
So passed a very sorry episode that continued to produce a great deal of personal distress, physical harm and death long after the last machine was shut down.
The demise of X-ray treatments meant that the use of electric needles was now the only sure method of permanent hair removal. Fortunately, in the 1940s, a quicker method than electrolysis began to become common. Known mainly as diathermy or thermolysis, it too was often described as being a ray. It was however, considerably safer.
See also: Thermolysis and the Blend
Updated: 12th July 2019
Sources
AMA Bureau of Investigation. (1929). The Tricho system: The Albert C. Geyser X-ray method of depilation. Journal of the American Medical Association, 92(3), 252.
Cleveland, D. E. H. (1948). The removal of superfluous hair by X-rays. Journal of the Canadian Medical Association, 59, 374-377.
Collins, P. (2007). Nothing but a ray of light. New Scientist, 195(2620), 68-69.
Beauty: Woman’s Most Precious Gift. [Booklet]. (n.d.). USA: The Dermic Laboratories.
Geyser, A. C. (1915). A resume of two hundred cases of hypertrichosis treated with the Roentgen ray. The Journal of Cutaneous Diseases Including Syphilis, 33, 520-524.
Geyser, A. (1918). Hypertrichosis. The Journal of Cutaneous Diseases Including Syphilis 36(1) 55-57.
Goodman, H. (1943). Your hair: Its health, beauty and growth. Garden City, NY: Halcyon House.
Herzig, R. (1999). Removing roots “North American Hiroshima maidens” and the X-ray. Technology and Culture. 40(4), 723-745.
Herzig, R. (2003). Situated technology: Meanings. In, N. E. Lerman, R. Oldenziel, & A. P. Mohun, Eds. Gender & technology: A reader (pp. 72-97). Baltimore: John Hopkins University Press.
Herzig, R. M. (2003). Plucked: A history of hair removal. New York: New York University Press.
Humphris, F. H. (1913). Electro-therapeutics for practitioners: Being essays on some useful forms of electrical apparatus and on some diseases which are amenable to electrical treatment. New York: Longmans, Green & Co.
Lapidus, S. M. (1976). The Tricho system: Hypertrichosis, radiation, and cancer. Journal of Surgical Oncology (8), 267-274.
MacFarlane Winfield, J. (1903). A brief history of the treatment of various forms of light and radio-therapy. Brooklyn Medical Journal 17(4), 163-167.
Martin, S., Strong, E., & Spiro, R. H. (1970). Radiation-induced skin cancer of the head and neck. Cancer, 25 (1), 61-70.
Morris, M., & Dore, S. E. (1907). Light and X-ray treatment of skin diseases. Chicago: W. T. Kenner & Co.
Sequeria, J. H. (1911). Diseases of the skin. London: J & A. Churchill.
Wolbach, S. B. (1909). The pathological histology of chronic X-ray dermatitis and early X-ray carcinoma. Journal of Medical Research, 21(3), 415-450.

Leopold Freund [1868-1943] used X-rays to treat a hairy mole. The report on this successful treatment was the start of the medical interest in using X-rays to remove hair.
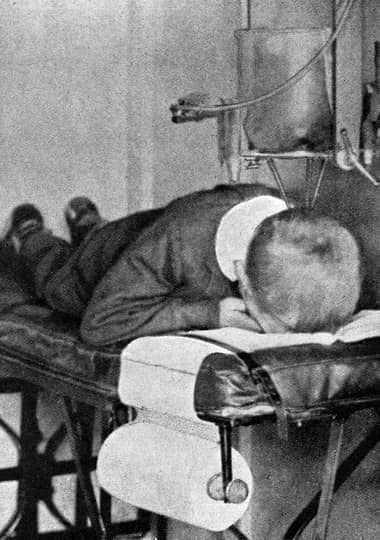
A young child receiving X-ray treatment for ringworm to induce hair loss (Sequeira, 1911). Epilation of the infected hair was once considered an important part of any treatment for many fungal skin infections and X-rays were used to cause the hair to fall out.
1917 Roebling Ray.
1920 Advertisement from Philadelphia claiming to use the Roebling Geyser Method. Clearly this refers to Frank Roebling Geyser and may indicate an early interest in commercialising what would later become the Tricho System.
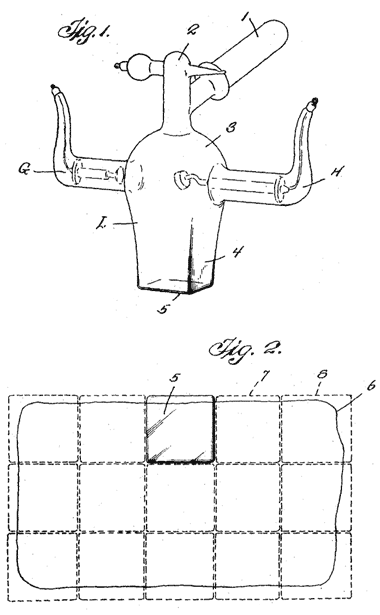
Two drawings from the US Patent submitted by Frank Geyser in 1924. Figure 1 shows the structure of the Cornell tube with its rectangular shaped window. Figure 2 shows the grid pattern the operator was to follow to avoid dosing the same area of skin twice.

Tricho Machine (Collins, 2007, p. 68).

Advertisment showing a drawing of the Tricho machine. “Clients sat at a mahogany cabinet with a small front window for the treatment area. The operators … threw a switch, and then – nothing happened, save for a faint hum and a whiff of ozone. After a few minutes the machine automatically shut off and the patient booked her next session.” (Collins, 2007)

William D. Coolidge [1873-1975] holding an example of the Coolidge X-Ray Tube he developed in 1913. The tubes gave operators a high degree of control over the intensity and energy of the X-rays it emitted. The tubes also functioned almost indefinitely.
1914 Marton Salons Cosmetiques with Dr. J. M. Marton (Consulting Chemist).
1922 Jules M. Marton. Advertisement for the Epilex-Ray Treatment in Chicago. He was not a graduate of any reputable medical school or licensed to practice medicine in the United States.
1922 J. M. Marton offering classes in ‘The art and science of facial chemistry’.
1923 The Dermic Institute.

1925 Tricho System.
1926 Tricho System. Although this is a poor quality image, the outlines of the Tricho machine can be made out.
1927 Tricho System. British advertisement using the actress Ann Pennington [1893-1971] as the model. The inference is that your face, underarms and legs should all be treated.
1927 Tricho System.
1929 Dermic Institute, here listed as using the Abbott-Marton Method.
1930 Dermic Institute.

1933 Hamomar Institute, another X-ray business.
1950 Vir-o-gen. This Pittsburg X-ray business was in operation from 1930 until at least 1951.
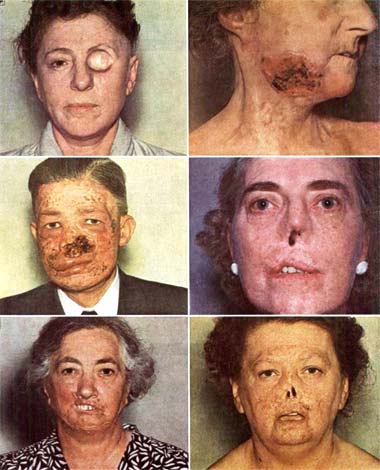
A range of facial cancers induced by medical X-ray treatments mainly for hirsutism and acne. The woman bottom right had received 100 X-ray exposures for acne. The woman bottom left had received 15 X-ray exposures for hirsutism. (Martin, Strong & Spiro, 1970)

A facial tumour from a 76-year-old female with a history of Tricho treatments some 30 years previous (Lapidus, 1976. p. 271).